Fetal surveillance and monthly prenatal exams are imperative to assist in the prevention of obstetrical emergencies. Fetal surveillance is even more crucial with a high risk pregnancy. The focal assessment in determining fetal health is the fetal heart rate (FHR). “The rationale for monitoring the fetal heart rate (FHR) is that FHR patterns are indirect markers of the fetal cardiac and medullary responses to blood volumes changes, acidemia, and hypoxemia, since the brain modulates heart rate” (Young, 2011). It is as if we are monitoring the fetus’s blood pressure, arterial blood gasses, oxygen saturation and central nervous system functions all from assessment of the heart rate. This is truly amazing and yet somehow archaic. The primary goal is early intervention in the event of fetal distress. Timely intervention can prevent hypoxic brain injury, as seen in cerebral palsy and/or prevent fetal death.
FHR can be assessed by auscultation with a fetoscope or a Doppler ultrasound stethoscope. Both of which are placed on the maternal abdomen. The fetoscope can pick up fetal heart tones at approximately 20 weeks gestation. Contractions can limit the use of the fetoscope. The Doppler stethoscope can detect a FHR at approximately 10 weeks gestation. The Doppler stethoscope is more commonly used, especially during labor. Doppler ultrasound is noninvasive and a common practice (Lippincott’s Nursing Procedures 2010). | 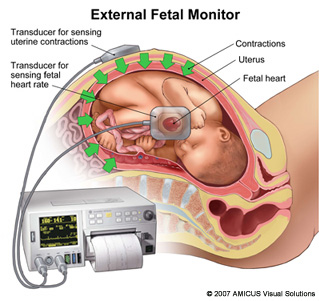 |
"Virtually all obstetrical organizations advise monitoring the FHR during labor” (Young, 2011). Also stated by Young is that there are studies that show that continuous FHR monitoring during labor does NOT reduce the risk of cerebral palsy or fetal death, yet is does lead to a higher rate of cesarean deliveries. “There is insufficient evidence to recommend for or against intrapartum electronic FHR monitoring for high-risk pregnant women” statement made by the United States Preventative Services Task Force (Young, 2011). Even with mixed scientific evidence, FHR monitoring during labor is a routine diagnostic tool in obstetrics. The fetal electrocardiogram is an invasive procedure as it measures FHR internally. An electrode is inserted transcervically and penetrates the fetal scalp to create a fetal ECG. Computer analysis can also be added to the ECG with fetal scalp blood samples to correlate the arterial pH with the ECG tracings. This has become the gold standard of FHR monitoring (Manning 2011).
The Nonstress Test (NST) is used to evaluate the FHR accelerations which are a normal element of fetal activity. The accelerations of the FHR equate to fetal movement and typical responses of the central and autonomic nervous system of the fetus. External fetal and uterine monitors are used to assess for fetal movement. A reactive (normal) NST should include two accelerations within 20 minutes, lasting 15 seconds or more with an increase in FHR of 15 bpm above baseline. Testing time can take up to 40 minutes. Parameters for a preterm fetus are similar with accelerations only lasting 10 seconds and 10 bpm above baseline. Testing time for the preterm fetus can last longer, up to 90 minutes. In a nonreactive (abnormal) NST, the above criteria are not met (Lippincott’s Nursing Procedures 2010). In the event of a nonreactive NST, it is recommended that the mother and baby receive further testing.
A Contraction Stress Test (CST), also known as an Oxytocin Challenge Test can be ordered. The CST induces uterine contractions to evaluate how the fetus will endure the pressure of labor. This is a test that should not be done on woman at risk for preterm labor, namely a history of preterm labor or having third trimester bleeding. Nipple stimulation is used to induce the natural production of oxytocin. If nipple stimulation does not bring on contractions, Pitocin is used via IV to induce contractions. Pitocin is a high risk drug that typically requires two RNs to cosign when administering. The goal is for three uterine contractions in 10 minutes without the effects of late deceleration on the FHR. A negative CST is considered reassuring. A deceleration with the contraction would be normal, although a late deceleration with more than 50% of uterine contractions is considered a positive CST or nonreassuring. There are other variable results depending on the variance of the decelerations of the FHR. If any variable decelerations are present, further testing is recommended.
Variable decelerations of FHR can be indicative of oligohydramnios. Amniotic fluid levels are also used to determine the well being of the fetus. This is tested via the biophysical profile (BPP). The BPP assesses the stability of the fetal central nervous system via five biophysical variables. For each variable listed below a score is given. A 2 is given for criteria that is met. A 0 is given if criteria is considered abnormal. 8-10 is normal. 7-5 is considered equivocal. 4-0 is abnormal. "The integration of the BPS into the management of high-risk obstetric patients has been associated with a significant reduction in perinatal mortality" (Manning 2011). The theory behind the BPS is that early recognition of possible acidemia or hypoxia is the best prevention of fetal demise. A modified biophysical profile consists of the amniotic fluid volume variable and the nonstress test. This requires far less time and "appears to be as reliable a predictor of long-term well-being as the full BPS" (Manning 2011).
The Nonstress Test (NST) is used to evaluate the FHR accelerations which are a normal element of fetal activity. The accelerations of the FHR equate to fetal movement and typical responses of the central and autonomic nervous system of the fetus. External fetal and uterine monitors are used to assess for fetal movement. A reactive (normal) NST should include two accelerations within 20 minutes, lasting 15 seconds or more with an increase in FHR of 15 bpm above baseline. Testing time can take up to 40 minutes. Parameters for a preterm fetus are similar with accelerations only lasting 10 seconds and 10 bpm above baseline. Testing time for the preterm fetus can last longer, up to 90 minutes. In a nonreactive (abnormal) NST, the above criteria are not met (Lippincott’s Nursing Procedures 2010). In the event of a nonreactive NST, it is recommended that the mother and baby receive further testing.
A Contraction Stress Test (CST), also known as an Oxytocin Challenge Test can be ordered. The CST induces uterine contractions to evaluate how the fetus will endure the pressure of labor. This is a test that should not be done on woman at risk for preterm labor, namely a history of preterm labor or having third trimester bleeding. Nipple stimulation is used to induce the natural production of oxytocin. If nipple stimulation does not bring on contractions, Pitocin is used via IV to induce contractions. Pitocin is a high risk drug that typically requires two RNs to cosign when administering. The goal is for three uterine contractions in 10 minutes without the effects of late deceleration on the FHR. A negative CST is considered reassuring. A deceleration with the contraction would be normal, although a late deceleration with more than 50% of uterine contractions is considered a positive CST or nonreassuring. There are other variable results depending on the variance of the decelerations of the FHR. If any variable decelerations are present, further testing is recommended.
Variable decelerations of FHR can be indicative of oligohydramnios. Amniotic fluid levels are also used to determine the well being of the fetus. This is tested via the biophysical profile (BPP). The BPP assesses the stability of the fetal central nervous system via five biophysical variables. For each variable listed below a score is given. A 2 is given for criteria that is met. A 0 is given if criteria is considered abnormal. 8-10 is normal. 7-5 is considered equivocal. 4-0 is abnormal. "The integration of the BPS into the management of high-risk obstetric patients has been associated with a significant reduction in perinatal mortality" (Manning 2011). The theory behind the BPS is that early recognition of possible acidemia or hypoxia is the best prevention of fetal demise. A modified biophysical profile consists of the amniotic fluid volume variable and the nonstress test. This requires far less time and "appears to be as reliable a predictor of long-term well-being as the full BPS" (Manning 2011).
Biophysical Profile
• Nonstress test-to assess for FHR acceleration with fetal activity
• Amniotic Fluid Volume-to assess for sufficient amount as indicator of fetal health
• Fetal Breathing Movements-assessing from length of episodes
• Gross Fetal Body Movements-to assess body and limb movement, including rolling
• Fetal Muscle Tone-to assess for active extension and flexion of spine, hands or limbs
• Amniotic Fluid Volume-to assess for sufficient amount as indicator of fetal health
• Fetal Breathing Movements-assessing from length of episodes
• Gross Fetal Body Movements-to assess body and limb movement, including rolling
• Fetal Muscle Tone-to assess for active extension and flexion of spine, hands or limbs